
Encounter Leads to Caring
February 27, 2025
AIDS Care Communities, Potrait of Community Participation in HIV and AIDS Issue
February 27, 2025Posyandu Must Not Be at The End of Its Rope
The existence of Posyandu in villages far from cities and district government centers is a key factor in successful village development, especially in improving the quality of maternal and child health. Therefore, the Posyandu program is being maintained. In fact, currently there is categorization of Posyandu to determine the form of support needed from various parties to improve the quality of services.
Considering the existence of Posyandu, in the second year of the Monitoring and Evaluation of the “Enhancing Civil Society Role to Achieve Quality Health Services System in East Sumba, Alor, and Malaka, East Nusa Tenggara” program, one of the aspects explored was policies regarding Posyandu, both at the district and village levels. In these three districts, there are no villages that do not have Posyandu, and there are even villages that have taken the initiative to open Posbindu services for youth and the elderly, although not as intense as the monthly Posyandu services. Based on interviews with the Health Office or Dinas Kesehatan (Dinkes), the Regional Development Planning Agency or Badan Perencanaan Pembangunan Daerah (Bappeda), and the Village Community Empowerment Agency or Dinas Pemberdayaan Masyarakat dan Desa (DPMD) of the three districts, the data on the number of villages and Posyandu registered with DPMD are as follows:

Table Number of Villages and Posyandu in 3 Regency in NTT
When looking at the ratio between the number of villages compared to the number of registered Posyandu, on average, each village has at least three to four active Posyandu units, with various service strata types. There are four strata of Posyandu: Posyandu Pratama, Posyandu Madya, Posyandu Purnama, and Posyandu Mandiri. Regarding the condition of all these Posyandu, each region has its own policies and unique approaches while remembering the vision and mission of regional leaders.
During discussions on the district government's priorities related to maternal and child health services through Posyandu, as well as discussing the uniqueness of related policies, the following responses from the Health Office of the three districts was as follows:
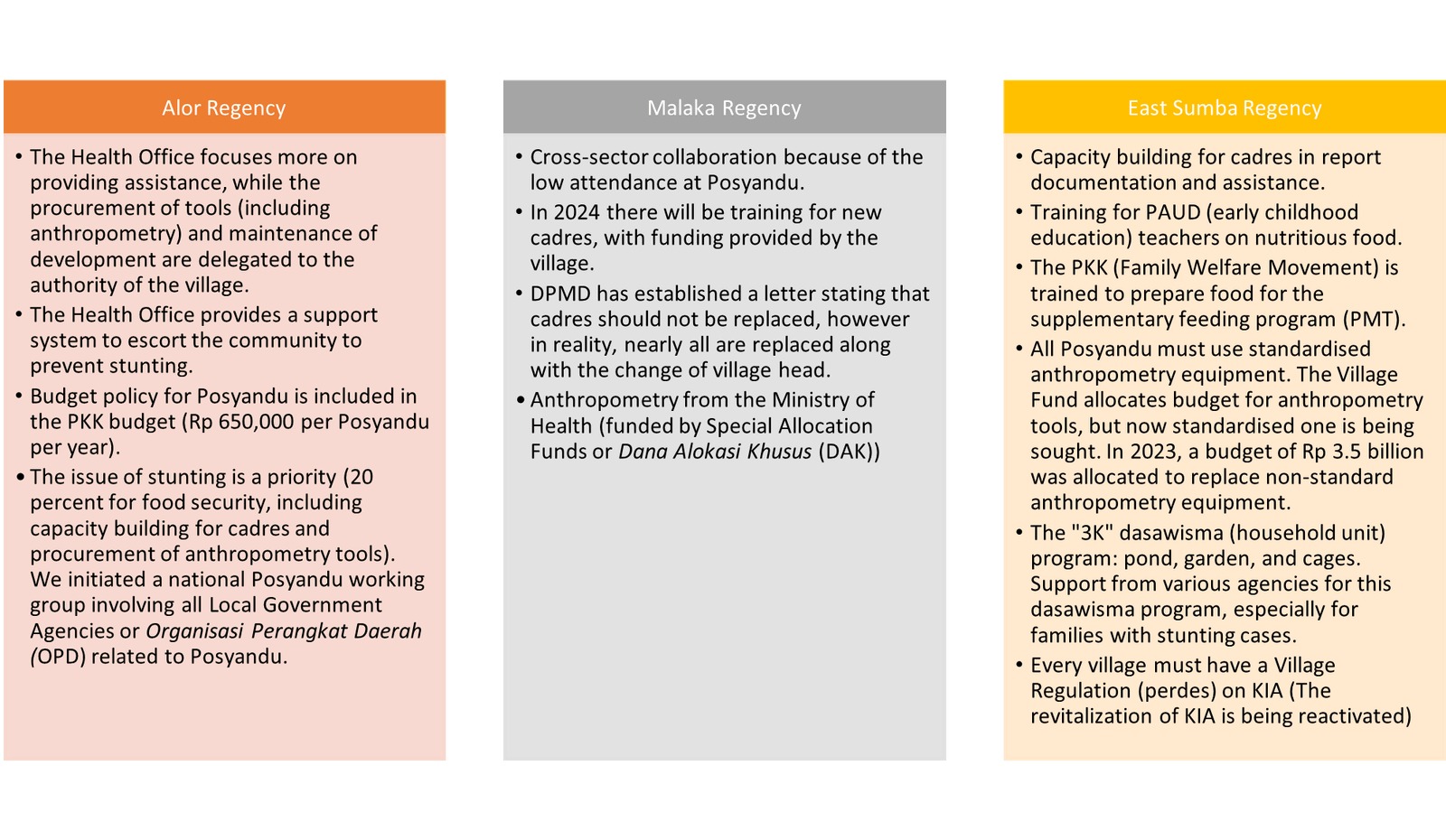
Response Table of Health Offices in 3 Districts
The policy priorities in these three regions seem to differ from one another, naturally because they are adjusted to the issues and potentials of each region, as well as the varying local budget and income capabilities. Each district government’s target in terms of basic health services through Posyandu are as follows:
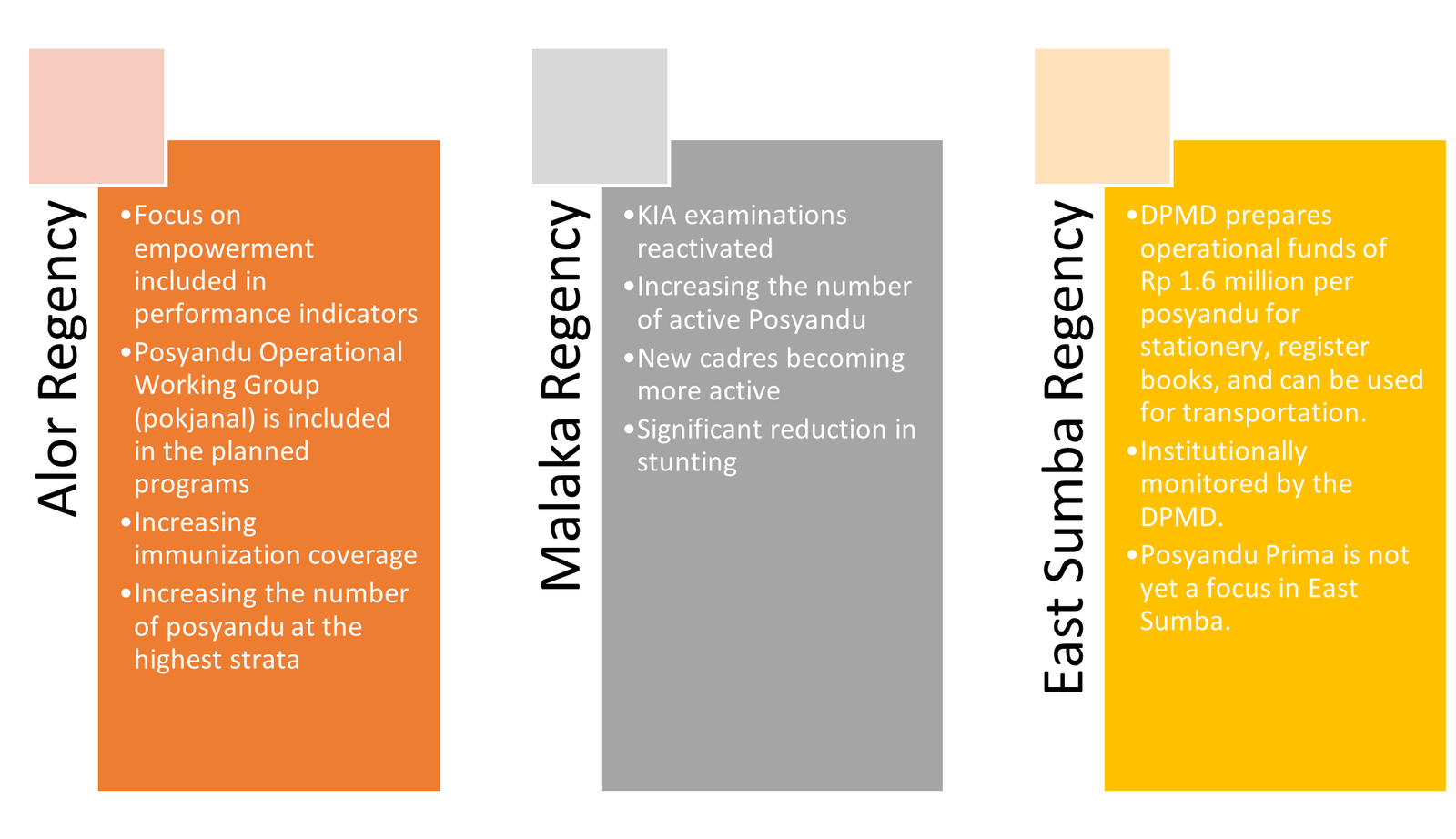
Government targets in basic health services through Posyandu

A father in Alor brings his child to Posyandu for weighing and receiving PMT.
In pursuing the realisation of these targets, the Health Office, as the main mandate responsible, is open to developing collaborations with other parties, including community-based organisations. No wonder when UPKM/CD Bethesda YAKKUM proposed a collaboration, the Health Office and related local government agencies (OPD) welcomed it. This collaboration on health service quality improvement programs encourages villages to take the initiative in health projects, supported by village resources, including funding regular Posyandu activities. Health initiatives that emerge from village governments and communities go beyond routine funding for supplementary food and cadre incentives; they also include new activities that were previously untouched.
Innovations that Differentiate the Assisted Posyandu
One aspect highlighted by interviewees about the differences before and during UPKM/CD Bethesda YAKKUM's assistance in the three villages is the implementation of the program in 30 villages was the emergence of health initiatives from the cadres, community, and the village government itself. Health initiatives are more focused on creating a variety of local food to make the supplementary feeding program (PMT) for toddlers and pregnant women more appealing. Selama ini, the PMT provided during Posyandu services was not varied, leading to disinterest among toddlers. In this regard, UPKM/CD Bethesda YAKKUM facilitated training for PKK mothers and Posyandu cadres on processing food ingredients so that PMT would be more appealing and parents could try cooking it at home. It is hoped that varying PMT with local ingredients from around the home will help toddlers enjoy the food and improve their nutrition. According to the Malaka Health Office, UPKM/CD Bethesda YAKKUM's intervention in supporting local food management must remain under the control of nutrition management personnel or Tenaga Pengelola Gizi (TPG) who work at each Puskesmas. This means that the preparation of local food menus for toddlers and pregnant women in each Posyandu service must be consulted with TPG, just as every family nutrition socialization in the village must involve TPG. In East Sumba, regarding food preparation at Posyandu, at least the PKK in the vilage is now involved in preparing local PMT. “At this stage, we start with training at the village level. PKK is trained to process food for PMT using local resources in their village. The village is given the freedom to process available ingredients like moringa. As per the governor's instructions, moringa must be used in local food. The cost of making moringa powder (23,000 rupiah) and snacks (16,000 rupiah) is covered. Undernourished and malnourished children are gathered at Posyandu and given PMT for up to 90 days," explained Mrs. Novri. She added that they are grateful to institutions like UPKM/CD Bethesda YAKKUM for their willingness to collaborate in educating and training PKK members and Posyandu cadres on local food processing variations.
Additionally, cadres and PKK mothers (who manage PMT) also learn to prepare healthy drinks to strengthen the stamina of pregnant women and the elderly so that during Posyandu for the elderly and pregnant women, they can consume and benefit from it. This is also important for reminding the elderly about traditional herbal drinks, knowledge of which has faded over generations. These simple health initiatives have triggered wider support, such as developing fish nurseries (supported by the Fisheries Department), planting vegetables and fruit as PMT ingredients, and even some psychosocially disabled individuals taking the initiative to provide food for PMT.

Counseling activities at Table 4 of the Posyandu service in Malaka
Another innovation in East Sumba, is that every Puskesmas, the Dharma Wanita of all OPD must have a fostered Posyandu. The Regent’s policy mandates that every official must have a foster child with malnutrition or undernutrition. Additionally, sub-districts are encouraged to innovate, such as with the "Jas Antik" (No Stunting Among Us) and "Selimut Cantik" (Save Mothers from Death in Childbirth) programs.
Responding to health initiatives at Posyandu, changes were observed by partners at the district level. As stated by Heri Zirr (DPMD of Alor Regency), Posyandu assisted in the UPKM/CD Bethesda YAKKUM areas are somewhat different from other Posyandu. For him, the activities facilitated by UPKM/CD Bethesda YAKKUM were beneficial and could even be expanded to small islands. To monitor Posyandu and health services in the village, policyholders created cross-department discussion groups, including DPMD and other OPDs. "What is interesting to me is that there is a change in cadre work motivation, and this time the village government is involved in Posyandu activities. Although the village is far and difficult to reach by health facilities, a pregnant women's class has been formed to educate them on maintaining their pregnancies," he explained.
Another difference, according to him, is that the village government has become increasingly aware of stunting issues after being involved in village-level stunting forums. Previously, discussions on stunting were limited to the district level [2], leaving many questions about stunting unanswered for village heads. Without understanding the long-term impact of stunting onthe village government did not immediately make policies to prevent and handle stunting children, the village government was slow to implement stunting prevention and treatment policies. However, after initiating stunting discussions at the village forum, this innovation successfully opened village heads' eyes to the urgency of preventing and accelerating the reduction of stunting. As of the interview, he mentioned that four villages had held stunting forums, with other villages being encouraged to do the same.
Another change observed by OPD was that what the government couldn't discover was found through village health initiatives, such as identifying cases of malnourished and undernourished toddlers. Rachmad Zainudin from Bappelitbangda Alor Regency shared that the discovery of malnutrition cases in North Mataru inspired the "Kekasih Kuning Program,"[3] which initially stemmed from UPKM/CD Bethesda YAKKUM's findings in the assisted village. This is very likely to happen in the future when village health workers, Puskesmas, and Posyandu cadres can manage valid data from increasingly high-quality Posyandu services.
Challenges in Developing Posyandu Services
Although the number of Posyandu continues to grow, its services improve daily with various policies and routine funding from Village Funds and support from various parties, Posyandu still faces its own challenges. On the positive side, these challenges should make Posyandu cadres and policymakers more creative in innovating. From observations by interviewees during monitoring and evaluation, there are several challenges that can be mapped out.
Despite the challenges and obstacles, Posyandu must evolve for the better. This is supported by policies that accommodate quality improvement, such as mandatory health service funding from Village Funds (30% for empowerment, including health), anthropometry support and capacity building from the Health Office through Puskesmas and other parties (NGOs, CSR, etc.). There are also cross-issue program policies (local food security, environmental health, agriculture, economic empowerment, etc.) that are mutually supportive and integrated. With innovations requiring village governments to work hard to improve Posyandu services, Posyandu should no longer be on the End of its Rope but rather strengthened and supported. Therefore, the regional vision of a healthy community and children free from stunting is increasingly optimistic about being realized.
Infrastructure and Facilities
Alor Regency
- There is no land available, especially in the sub-districts.
- The pioneer posyandu has no supporting facilities resulting in attendance rates of pregnant women and toddlers being significantly below average.
- Inclusive health facilities: some puskesmas and hospitals have, but posyandu have not, it is important to think about it, learn from the Puskesmas and posyandu in Besikama, must be campaigned.
Malaka Regency
Some have their service building but do not have tables, chairs, or furniture, while furniture is the responsibility of the village government.
East Sumba Regency
- Not all village heads understand their responsibilities for providing infrastructure and facilities.
- The registration and supply of KIA books from the Ministry of Health, currently limited, not all targets of pregnant women get KIA books so that the General Allocation Funds or Dana Alokasi Umum (DAU) will print KIA books because this supports the SPM in the health sector (specific grant)
Good Governance
Alor Regency
- Replacement of village head cadres was also replaced due to Village Head Election or Pemilihan Kepala Desa (Pilkades).
- DPMD has difficulty measuring the level of community participation.
Malaka Regency
- Many cadres were replaced with the new village head.
- Cadres (especially those newly elected) have not been able to deliver education.
- The village head is oriented towards physical development, not empowerment. The level of participation is still a problem. For example, the Posyandu has ten cadres, but the village government rarely attends, and the average active cadre is only three.
East Sumba Regency
- Trained cadres are transferred or replaced.
- The Health Office's intervention through the Puskesmas does not look at the distance of the posyandu, but has not been able to roam all villages on a regular basis.
Motivation and Service
Alor Regency
- There are 3Ts : late to reach the health facility, late decision, late treatment.
- Awareness of bringing children and pregnant women to Posyandu for examination is not 100% (only 60%)
Malaka Regency
- PMTs are on display, but no education is given on how to feed children under five years old properly
- The attendance rate of children under five to Posyandu has not reached 100%, only 92.12%
- Children come to Posyandu already full, so they refuse to eat PMT.
- There are actually many private sector aids for local food, but they don't know about it, so they don't access it.
- Services for pregnant women and toddlers with disabilities still exist but are home visits, not brought to the Posyandu location point
East Sumba Regency
- Pregnant women with disabilities do not come to ANC, puskesmas has a budget for visits to pregnant women with disabilities, immunization sweeping. visited home
- Routine attendance target: 100%, but when it's not a weighing operation, there must be someone lost so they are visited.
- AKB (Infant Mortality): 33 cases in 2021, 88 cases in 2022—a sharp increase due to the lack of equipment in community health centers and budgeting for procurement. In 2023: 17 cases.
- The high AKI (Maternal Mortality) and AKB factors include 3 delays: delays in reaching health facilities, delays in decision-making, and delays in receiving treatment. Each maternal death is required to be audited. In Sumba, there is a hierarchical structure, so the lower class waits for decisions from their superiors.
(Dewi Utari)
References:
- Interviews with Alor District Health Office (Ezron Maro as Secretary of the Office, Gusman Lalangpuling as Maternal and Child Health management staff in the Public Health Division), Rachmad Zainudin as a functional planner intermediate expert of Bappelitbang, and Herri Sir, Head of Community Empowerment Division of DPMD. In Malaka District with the Health Office (Desriana D.M.Feran in the P2P section and Ignatius Manik Un, as coordinator of the immunization and surveillance program, Maria Gaudensiana H. Taek, in the Kesmas section of Promkes and Posyandu), Bappeda namely Anton Bere Mali, functional planner and the PMD Office namely Matilde Niis Seran as Secretary of the Office, Rosa Brito as Head of the Community Participation and Village Potential Development Section and Asince Bria as an implementer of the Sosbud Division. In East Sumba District, interviews with the Health Office (Novri Kilimandu as Head of P2P and Juleha Keliwawa as an administrator in the Yankes field), and Bappeda namely Benyamin L. Ama as an implementer of the Human Development Government Sector.
- Presidential Regulation No. 72/2021 on the Acceleration of Stunting Reduction that is holistic, integrative, and quality through coordination, synergy, and synchronization among stakeholders. This Presidential Regulation is a replacement for Presidential Regulation Number 42 of 2013 concerning the National Movement for the Acceleration of Nutrition Improvement. In addition, Presidential Regulation 72 of 2021 ensures that village governments coordinate and fund the acceleration of stunting reduction at the village level, not just at the district/city level.
-
Moringa planting movement program to overcome malnutrition and undernutrition among toddlers and pregnant women


